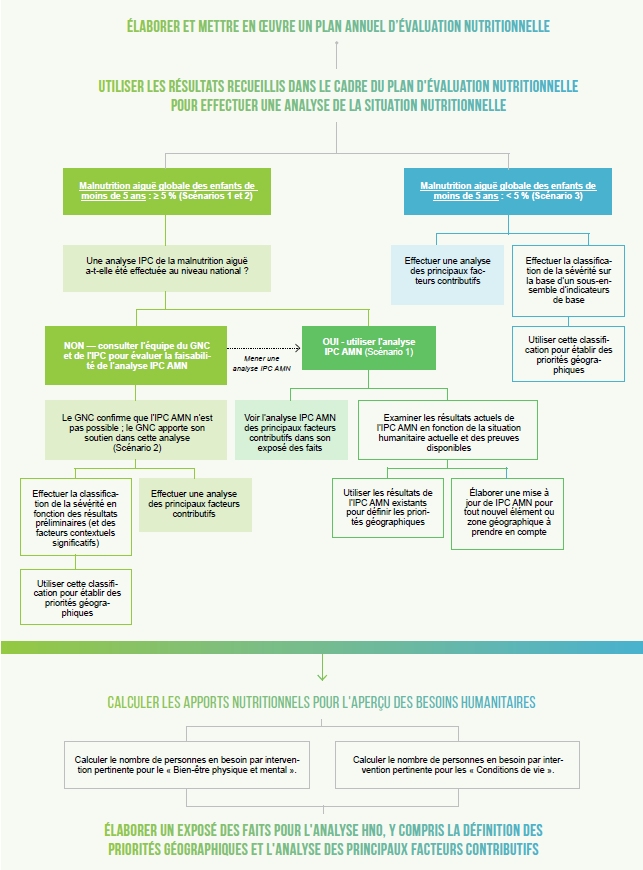
The starting point for any HNO analysis in the nutrition sector is to use the strongest, most recent outcome-level data available. Ideally, this means data collected within the last 6 months, and not older than 24 months.
Priority data sources include:
- Household surveys such as SMART surveys, which provide GAM prevalence rates at the admin 3 level (or equivalent).
- IPC Acute Malnutrition (AMN) analysis, if it covers most of the country and is up to date.
If outcome-level data are absent, incomplete, or outdated:
- Use proxy indicators, such as MUAC screening data, dietary diversity, IYCF practices, morbidity rates, or micronutrient supplementation coverage.
- Explore alternative data sources, for example: health facility reporting systems, nutrition surveillance systems, rapid assessments, or campaign-based data.
- Always document clearly when and why proxy or alternative sources are used.
Further technical guidance on the use of alternative data sources is available in the GNC Needs Analysis Guideline and in dedicated GNC webinars (EN, FR and SP).
Note: always start with the best outcome-level data you can find. If it’s missing or outdated, you can fall back on proxies and alternative sources - but you must be transparent about what you’re using and why.